
Research Article | DOI: https://doi.org/10.31579/2578-8965/009
Obstetrics & Gynecology Department - Faculty of Medicine- South Valley University
*Corresponding Author: Abd El-Naser Abd El-Gaber Ali, Obstetrics & Gynecology Department - Faculty of Medicine- South Valley University. Email: ayman_gamal007@yahoo.com
Citation: Abd El-Naser Abd El-Gaber Ali , Khaled M Abdallah , Ahmed Abdelhamid, Sildenafil Citrate versus Nifedipine and Dydrogesreone in Prevention of Preterm Labor with Short Cervix .J. Obstetrics Gynecology and Reproductive Sciences, 2(1); DOI: 10.31579/2578-8965/009
Copyright: © 2018 Abd El-Naser Abd El-Gaber Ali et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 April 2018 | Accepted: 07 May 2018 | Published: 08 May 2018
Keywords: Sildenafil citrate – Nifedipine – Dydrogesrone - Preterm labor – Short cervix
Background: Prevention of the premature birth occurrence remains is considered one of the most tough challenges for obstetricians worldwide, mainly to avoid neonatal prematurity complications leading to short and long term morbidities additionally prematurity prevention will reduce premature neonatal mortality rates which is considered a major health concern of obstetricians, neonatologists and families.
Objective: To compare and contrast the efficacy of Sildenafil citrate, Nifedipine and Dydrogesrone in prevention of premature labor in gestations with short cervix.
Setting: Obstetrics & Gynecology Departments, Faculties of medicine, south Valley and Al-Azhar (Asyut) Universities, Egypt.
Duration: from September 2014 to March 2018.
Patients And Methds: the study was conducted on 300 pregnant women who randomly divided into three groups: Group I included 100 cases received Sildenafil citrate (Respatio tablet 20mg twice daily orally), Group II included 100 cases received Nifedipine (Epilat retard tablets 20mg twice daily orally) and Group III included 100 pregnant women received dydrogesreone 10 mg (Duphaston) twice daily orally.
Results: incidence of preterm labor was (9.37, 8.51 and 14.28) in (Group I, Group II and Group II) respectively. Mean ± SD of cervical length at 32 weeks of gestation was mildly statistically significant among groups (p value <0.05) but no significance in neonatal outcome (p value >0.05) except birth weight which had a highly statistically significant difference (p value < 0.001). There was a highly statistically significant difference among studied groups as regard to drug side effects in (p value <0.001).
Conclusion: Sildenafil citrate was as effective as Nifedipine and better than oral Dydrogesterone on myometrial relaxation and prevention of preterm birth in pregnant women who had short cervix.
Reccommendation: Sildenafil citrate could be one of the most successful agents in prevention of preterm labor in threatened preterm cases.
Preterm labor is defined as delivery of fetus after 20 weeks and less than 37 completed gestational weeks. Preterm birth is always a major obstetric healthcare issue worldwide [1,2]. It represents a major cause of neonatal, infant and child death and disability up to age of 5 years in the developed world and represents the leading cause of perinatal mortality and morbidity in the whole world [3&4], about fifteen million premature neonates are born every year globally, and a million of them die because of prematurity complications [4,5]. Preterm babies are at greater risks of grave perinatal morbidities [6, 8]. Although many babies delivered prematurely had a normal and completely healthy life, some significant proportion experienced life-long disabilities and health issues [9]. The chief dilemma of premature births is its negative impact on neonates themselves, their families, and society as a whole in which there is significant healthcare costs due to perinatal health issues and long term disabilities [1, 4, 7, 10]. Prevention of preterm labor has the priority in health care system programs since preventive measures are superior than treatment protocols [11].
Prevention of preterm labor to be successful requires multiple approaches including public health efforts with educational health programs, modification of patient lifestyle, optimal obstetric protocols of healthcare, efficient approaches for prediction and diagnosis of threatened and established preterm labor and implementation of effective, tailored case management pathways according to case scienario [12]. Preconception intervention modalities e.g weight reduction in obese female population, nutritional supplementation for underweight women, and cessation of smoking have a favourable impact on premature birth rates and its clinical sequelae [13,14]. Dydrogesreone is a progesterone stereoisomer acts at biochemical level as a selective progestin with a high receptor affinity, due to its retro-structure that binds to the progesterone receptor. Dydrogesreone is safe and have well acceptable tolerability. It is similar to natural progesterone hormone in molecular structure and pharmacological properties with sufficient oral bioavailability. 2–5 hours is the maximum time required for Dydrogesreone to reach peak plasma concentration levels after oral intake, 20 mg/day of Dydrogesterone is equivalent to 200mg of progesterone administered vaginally [15]. Nifedipine is a calcium channel blocker that could be used as an key tocolytic agent [16, 17]. The most substantial updated Cochrane review [18] concerning calcium channel blockers displays that it could be used for tocolysis in prevention of acute threatened preterm delivery according to different 12 RCTs (10 of them used Nifedipine) 1029 patients were recruited in these trials. This review had concluded that, as comparison to any other tocolytic agent (as beta-mimetic mainly), calcium channel blockers (Nifedipine mainly) could diminish the hazardous risk of premature labor within 7 days of administration. Sildenafil citrate in fact enhances smooth muscle relaxation by preventing cGMP degradation (the second messenger) by phosphodiesterase enzyme (PDE5) [19,20]. Moreover, the BKCa channels had been implicated by direct or indirect fashion in the sildenafil mode of action [21, 22].
The aim of this research study is to compare the effectiveness of different tocolytic agents (Sildenafil citrate, Nifedipine and Dydrogesreone) in prevention of premature labor in gestations with short cervix.
The study was performed on 300 gestations from those visitingto Obs fetal medicine units of Obstetrics & Gynecology departments at South valley and Al-Azhar (Asyut) University Hospitals in the period from September 2014 to March 2018. Inclusive research criteria; 19 – 40 years old, BMI < 30> included 100 pregnant women received oral Dydrogesterone 10 mg (Duphaston) twice daily orally. To fulfill the target number of cases for this study (300 cases), we actually examined about 5000 pregnant women at mid-gestation.
(1) Full clinical history taking including meticulous menstrual history for precise estimation of expected date of delivery (2) Full clinical physical examination and assesment, involving general, obstetric and local examinations (3) laboratory investigations e.g CBC, RBS, kidney and liver function tests (4) Sonographic examination and assesment: (a) Trans-abdominal sonography for fetal biometry (including BPD, HC, FL and AC), placental site and grading, amniotic fluid volume, fetal anomalies (b) Trans-vaginal sonography for cervical length (CL) measurement (at 24, 28 and 32 weeks of gestation).
Recruited subjects were allocated randomly into 3 research groups by using a computer-generated randomization system (Microsoft office excels, 2010). The randomization list was hidden, expressed by sequential numbers and sealed in opaque envelopes just before start of allocation. Each number was linked to a ready prepared pack which contained sildenafil citrate (Respatio 20mg), calcium channel blocker (Epilat retard 20mg) or Dydrogesterone (Duphaston 10mg). The process of packing, numbering and sealing were performed by 2 different persons other than the investigator. Both investigator and observer were not aware about which drug cases had received (double-blinding).
Follow up: (a) All patients were followed up every two weeks until time of delivery and for one week later (b) Any episodes of premature labor contractions were clinically assessed carefully and recorded (c) If manifestations of threatened preterm labor progressed and not controlled with the regimen in this study, the patients were admitted to the hospital and magnesium sulphate in intravenous drip was commenced in a dose of 6 g in 500 ml glucose 5% and repeated every 6 hours till premature uterine contractions have resolved (d) Any complications developed were recorded. During follow up 12 cases dropped from the study (4 cases in group I, 6 cases in group II and 2 cases in group III) due to difficult communications or departure outside the area of study so the final number of cases continued in the study was 288 cases that delivered at South Valley and Al Azhar universities hospitals. Data of all patients finally was collected, tabulated and statistically analyzed.
Statistical analysis:
Data management and analysis were performed using Sigma Stat program; version 3.5 The Figures were done using Microsoft Excel. Data were statistically described in terms, mean±standard deviation (±SD) or number and percentage. Comparisons between categorical variables were done by the chi-square test. P-values was considered significant if <0>
Incidence of preterm labor was (9.37, 8.51 and 14.28) in (Group I, Group II and Group II) respectively (table 3). Mean ± SD of cervical length at 32 weeks of gestation was statistically significant among studied groups with p value > 0.05 (table 2). There was a highly statistically significant difference among the 3 groups in birth weight with p value <0.001 (figure 1) but there was no statistically significant differences as regards TTN, RD, NICU or neonatal death (figure 2) with p value > 0.05. There was a highly statistically significant difference among studied groups in drugs side effects as headache, hot flushes and palpitations with p value< 0.001 (figure 3).
Group I (Sildenafil citrate) N=100 |
Group II (Nifedipine) N=100 |
Group III (Dydrogesterone) N=100 | ANOVA | ||
| F | P-value | ||||
Maternal agein years(Mean ± SD) | 25.03±6.50 | 27.23±6.05 | 27.86±7.54 | 1.466 | 0.237 |
| BMI in kg/m2 (Mean ± SD) | 25.46±2.65 | 24.84±2.73 | 25.56±3.20 | 1.474 | 0.147 |
| Parity (Mean ± SD) | 1.60±1.79 | 1.83±1.96 | 1.53±1.96 | 0.204 | 0.816 |
P value>0.05
Table (1): Demographics data of the 3 studied groups
Group I (Sildenafil citrate ) N=100 |
Group II (Nifedipine) N=100 |
Group III (Dydrogesterone) N=100 | ANOVA | ||
| F | P-value | ||||
Cervical lengthat 24 weeks (mm) (Mean ± SD) | 14.96±2.15 | 14.96±2.44 | 15.80±3.38 | 0.943 | 0.393 |
Cervical lengthat 28 weeks (mm) (Mean ± SD) | 13.13±2.09 | 12.70±2.26 | 12.26±4.37 | 0.591 | 0.556 |
Cervical lengthat 32 weeks (mm) (Mean ± SD) | 12.60±1.75 | 12.57±2.24 | 11.03±2.29 | 4.231 | 0.019* |
Table (2): Comparison between the 3 research study groups concerning cervical length measurement at 24, 28 and 32 gestational weeks
Gestational age | Studied Groups | ||||
Group I (Sildenafil citrate) | Group II (Nifedipine) | Group III (Dydrogesterone) | Total | ||
< 37weeks> | N | 9 | 8 | 14 | 31 |
| % | 9.37% | 8.51% | 14.28% | 10.72% | |
| ≥ 37weeks | N | 87 | 86 | 84 | 66 |
| % | 90.63% | 91.49% | 85.72% | 89.28% | |
| Total | N | 96 | 94 | 98 | 288 |
| % | 100.00 | 100.00 | 100.00 | 100.00 | |
| Chi-square | X2 | 6.467 | |||
| P-value | 0.038* | ||||
Table (3): Incidence of preterm labor in the 3 studied groups
* statistically significant
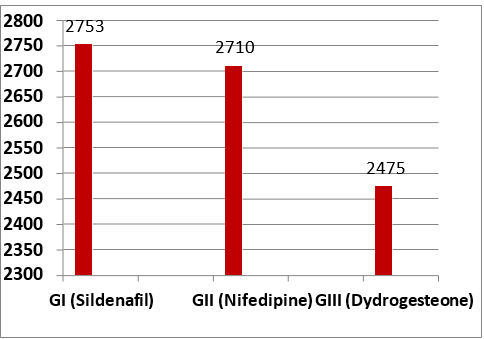
Figure (1): comparison between 3 research groups as regards neonatal birth weight in grams
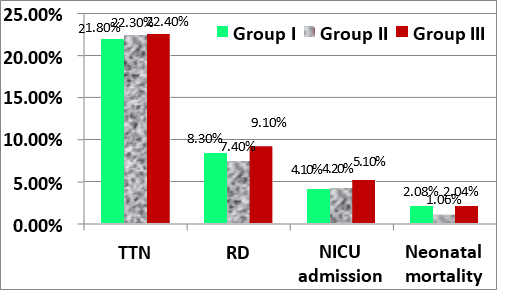
Figure (2): comparison between 3 research groups as regards, transient tachypnea of new born, respiratory distress, neonatal intensive care unit admission and neonatal mortalities
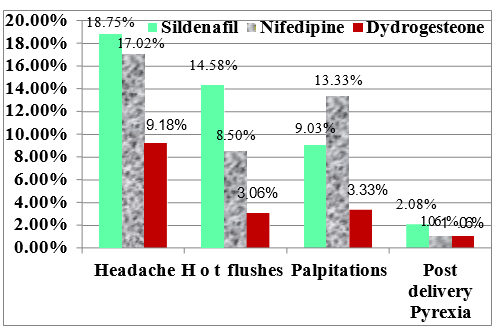
Figure (3): Drugs side effects in the 3 studied research groups
Premature birth is one of the chief etiologies of perinatal mortality and disability in pediatric population principally correlated to the birth <34>
Drugs adverse effects were statistically significant among the 3 studied groups we had found that headache, palpitation and hot flushes more obvious in group I and II but less in group III (figure 3). Many previous studies had been discussed the efficacy of progesterone, calcium channel blockers or any of the other tocolytics in prevention of threatened preterm labor, from those studies, Ladan et al. [24] studied the comparative efficiency between Nifedipine and intramuscular progesterone, the success rates with intramuscular progesterone and oral Nifedipine were 83% and 82.7%, respectively but there was no a statistically significant difference in the previously mentioned 2 agents concerning the gestational age at time of delivery, mode of delivery, neonatal birth weight, in the rate of NICU admission and hospitalization period, These results and findings were in harmony with that reported in our study as regards to neonatal outcome but in our study the prevalence of preterm labor was higher in Dydrogesterone than Nifedipine this may can be explained because of the route and type of progesterone was different from that used in Ladan et al. The mechanisms of progesterone in prevention of preterm labor is by maintainance of uterine quiescence by varioust actions such as relaxation of uterine smooth muscle, blocking oxytocin action, prevention of the gap junctions formation, reducing the oxytocin receptors concentration in uterine smooth muscles and inhibiting the production of prostaglandins by amnion, chorion and decidua [25]. In a study performed by Wilasinee and Vorapong, [26] as the study had compared oral dydrogesreone (20 mg daily) and placebo in a randomized double blinded controlled trial, the study results were (Rates of recurrent uterine contractions in both groups were 87.5% versus 91.7%, p value was 0.64 and there were no differences in latency periods between both groups 32.7 ± 20.2 days versus 38.2 ± 24.2 days with p value was 0.39 so Wilasinee and Vorapong, study recommended that adjuvant treatment with oral Dydrogesterone 20 mg/day could not decline the rate of recurrent uterine contractions and prolong latency periods in preterm birth management in comparison with placebo and these findings agreed with our study results. But in another study reported by Bomba-Opon et al. [27] that was a retrospective review of usage of 200 mg progesterone vaginally after tocolysis by fenoterol or verapamil in threatened preterm birth and had found that it was associated with prolongation of gestational period in comparison to no medication (7.6 versus 6.3 weeks with p value was 0.039).
In this study we selected dydrogesterone for investigation in order to overcome the disadvantages of oral progesterone that has a wide range variability in absorption and bioavailability among different individuals. Also about the dose 20 mg/day we had selected
because it had an equivalent dose to 200 mg of vaginal progesterone as mentioned in Ariea et al.’s study [28]. In Systematic review and meta-analysis reported by Agustín et al. [29] 26 trials that involving 2179 women were included. Nifedipine had been associated with a significant decline in the risk of preterm labor within 7 days of starting of treatment (relative risk, 0.82; 95% confidence interval , 0.70–.097) and < 34>Raheela et al.[30] had found that, myometrial relaxation caused by sildenafil citrate was a concentration-dependent manner, the relaxation of uterine muscles in presence of 20 mmol/L of tetraethyl-ammonium was statistically significantly different (p value <0>Sher and Fisch study [31].
Sildenafil citrate could be one of the most successful agents in prevention of premature labor in cases with threatened preterm labor more than Dydrogesterone with less palpitation occurrence than Nifedipine.
A future randomized controlled trial with larger sample size and Sildenafil citrate greater dosage should be used for better evaluation of the benefits and adverse effects on fetus and mothers in case of its prophylactic use in
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
